CALL US NOW :
(716) 772-7500
EMAIL ADDRESS :
info@drkaplansky.com
LOCATION ADDRESS :
8038 Rochester Rd. Gasport NY
(716) 772-7500
info@drkaplansky.com
8038 Rochester Rd. Gasport NY
If you have been declined for implants because of severe upper-jaw bone loss, that conversation may not have considered zygomatic implants. Dr. Igor Kaplansky, DDS — ZAGA Center Certified, Diplomate ABOI/ID, and co-author of the zygomatic implant clinical textbook — evaluates every case from a CBCT scan. The cheekbone anchor makes a fixed full arch possible without bone grafting.
ZAGA Center certification requires advanced clinical training, verified case volume, and peer review by the international ZAGA Zygoma faculty — not a marketing designation.
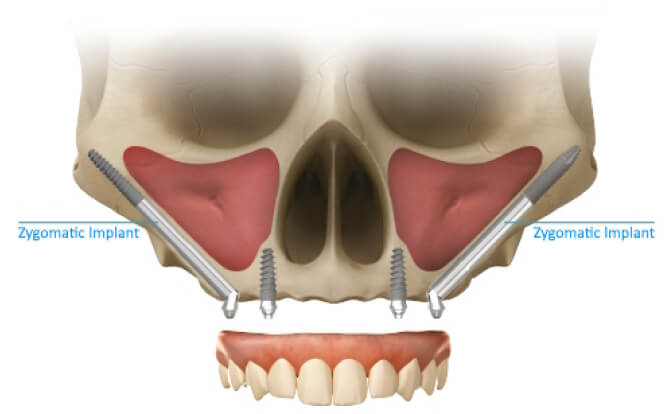
The zygomatic bone retains its density regardless of jaw bone loss, so we anchor a fixed full arch in the cheekbone — bypassing the 6–9 month bone grafting timeline entirely.
Dentistry by Dr. Kaplansky is 1 of 11 ZAGA Centers in the United States, out of approximately 60 worldwide. Patients travel here from across Gasport, Lockport, Buffalo, Niagara Falls, and Rochester for this procedure.
A bone graft can restore enough volume for standard implants — but it adds a separate surgery, a 6–9 month healing period before implants can be placed, and the risk that the graft will not integrate. Zygomatic implants bypass the deteriorated upper jaw entirely by anchoring four to five times longer into the cheekbone, which does not resorb after tooth loss. For patients who have waited months or years for a solution, this often means receiving permanent upper teeth months sooner than the grafting pathway would allow.
Anchored in the dense cheekbone, zygomatic implants skip the graft surgery and the 6–9 month integration period it requires.
Zygomatic anchorage is engineered for cases where standard implants and grafts are not viable — including patients with prior implant failure or sinus involvement.
Every case is anatomy-guided and performed by Dr. Kaplansky — one surgeon, every visit, never a rotating associate.

Laura had been declined for implants at multiple practices because of severe upper-jaw bone loss. She traveled for a CBCT consultation with Dr. Kaplansky, who identified her as a candidate for upper zygomatic implants paired with a lower TeethNow zirconia arch. After a single planned surgery and a smooth recovery, she was restored with permanent zirconia teeth — the same outcome other providers had told her was no longer possible.
The ZAGA approach treats every upper-jaw case as anatomy-specific. When zygomatic anchorage alone is not the right answer, Dr. Kaplansky may recommend trans-sinus, trans-nasal, or pterygoid placement — each planned from your CBCT, each documented in the zygomatic implant textbook he co-authored.
For posterior upper-jaw atrophy, a trans-sinus implant is guided through the maxillary sinus along a CBCT-planned path. It restores anchorage in cases where a sinus lift and graft would otherwise be required — and where the time to a fixed restoration matters.
When anterior maxillary bone is too thin for standard placement, a trans-nasal implant engages the dense nasal floor. The result is a stable foundation for the front of the upper arch — restoring full lip support and a natural smile line.
The pterygoid plate is the densest bone at the back of the upper jaw. Anchoring there delivers immediate stability for the rear of a full-arch restoration, avoiding sinus lifts entirely — a technique Dr. Kaplansky has documented in the clinical literature.
If another practice has told you that you are not a candidate for implants, that opinion may not have considered the remote anchorage options above. A CBCT-based second opinion at Dentistry by Dr. Kaplansky takes one visit and produces a written candidacy assessment you can keep.
Every case follows the same anatomy-guided four-stage path. Dr. Kaplansky personally reviews your CBCT scan, designs the surgical plan, places the implants, and oversees the restoration — no rotating associates.
Your consultation includes a CBCT scan. Dr. Kaplansky personally reviews the 3D anatomy of your upper jaw, cheekbone, and sinuses before making any recommendation.
Using the ZAGA Zygoma Anatomy-Guided Approach, every implant trajectory is mapped to your individual maxilla — not a standardized protocol.
Long zygomatic implants are anchored in the cheekbone under IV sedation, bypassing the deteriorated upper jaw and the need for any bone grafting.
Once the implants integrate, your final full-arch zirconia prosthesis is placed — the same TeethNow zirconia system used for non-zygomatic cases.
















492 pages of clinical technique
800+ surgical and anatomical images
1,000+ peer-reviewed references
Dr. Kaplansky is a co-author of this clinical textbook on remote anchorage implant technique. The volume features one of his combined cases — zygomatic, pterygoid, and incisive canal implants placed alongside a full-arch zirconia restoration. This level of academic contribution is rare even among experienced implant dentists.










Zygomatic implants are long dental implants — typically four to five times the length of standard implants — anchored in the zygomatic bone (the cheekbone) rather than the upper jaw. They make a fixed full arch possible for patients with severe upper-jaw bone loss who do not have enough bone for standard implants.
You may be a candidate if you have been told you cannot receive implants due to insufficient upper-jaw bone, if you have experienced prior implant failure due to bone loss, or if you want to avoid multiple bone grafting surgeries and the 6–9 month healing period they require. Candidacy is confirmed by a CBCT scan reviewed by Dr. Kaplansky.
No. Zygomatic implants bypass the deteriorated upper jaw entirely by anchoring in the cheekbone, which retains its density regardless of jaw bone loss. There is no graft, no graft healing period, and no uncertainty about whether the graft will take.
Zygomatic implants are designed for permanent function. The cheekbone anchor does not resorb the way a compromised upper jaw does, and long-term outcomes are comparable to standard implants when performed by a ZAGA-certified specialist.
Zygomatic implant cases typically start in the $36,000–$55,000 per-arch range, reflecting the specialized training and case complexity required. We accept CareCredit, offer in-house financing, and verify your insurance benefits before treatment. After your CBCT-based candidacy review, you receive a written estimate that itemizes surgery, sedation, and the final zirconia prosthesis — no surprises later.
If another practice has told you that you are not a candidate for dental implants, the right next step is a CBCT-based second opinion from a ZAGA-certified specialist. Patients travel to Dentistry by Dr. Kaplansky from across Gasport, Lockport, Buffalo, Niagara Falls, Rochester, and beyond for this evaluation. Call (716) 772-7500 or book online — you will leave with a written treatment plan, not a sales pitch.
Still deciding about your treatment options? Share your contact info, and we’ll reach out to answer your questions.
You’ll also receive a free copy of Dr. Kaplansky’s A Patient’s Guide to Dental Implants eBook to help you make an informed choice.

