


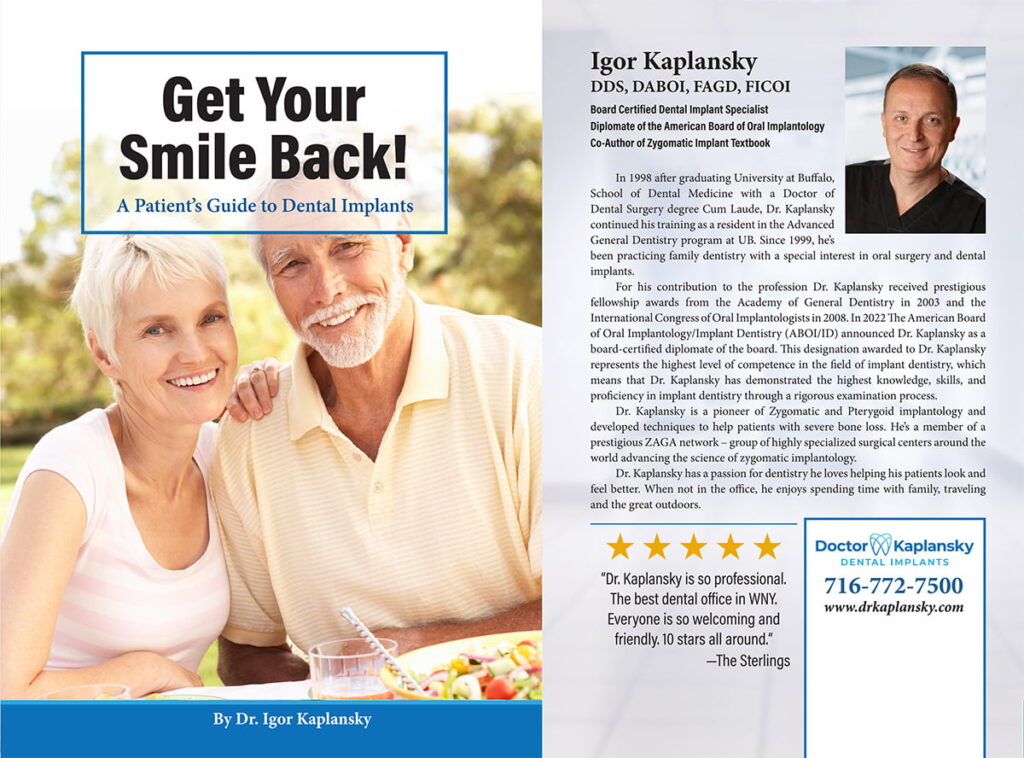


Dr. Igor Kaplansky, DDS
Diplomate ABOI/ID · Fellow AAID, FICOI, FAGD · ZAGA Center Certified
Board-certified implant specialist and ZAGA-certified zygomatic surgeon. One of fewer than 600 dentists nationally with Diplomate-level credentials in oral implantology, and one of 11 ZAGA Centers in the United States.